Q12. Do patients with Kallmann syndrome grow to normal height ?
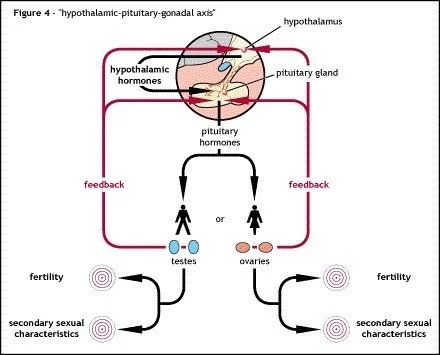
During puberty growth is controlled primarily by two hormones; growth hormone and testosterone in males and growth hormone and oestrogen in females.
During puberty growth hormone, along with a couple of other hormones act on the bones to cause them to grow so the body can reach its genetically pre-determined adult height. Bones are living tissue and are affected by the actions of hormones, just like any other tissue in the body.
The long bones (femur / thigh bone and humerus / upper arm bone) grow to their correct length under in the influence of growth hormone. Normally at puberty oestrogen or testosterone causes the end plates of these bones to fuse and harden to prevent any further growth.
If for any reason oestrogen or testosterone are missing, as in Kallmann syndrome, the bones do not stop growing and continue past their pre-determined length. This means that some patients with Kallmann syndrome, especially when un-diagnosed are above average height and can appear to have longer arms in relation to the rest of their body.
Take a look at the cross-section of a femur in Figure 11. A bone is made up largely of porous tissue. Calcium and Vitamin D are required to ensure the bone retains its strength while it grows under the influence of growth hormone. Calcium is mainly obtained through the diet via dairy products while Vitamin D is formed when skin is exposed to direct sunlight.
Changes in bones structure during puberty.
During puberty testosterone in males and oestrogen in females works alongside growth hormone to increase bone strength by depositing more calcium within the bone with the aid of Vitamin D, this is known as calcification.
A bone grows mainly lengthwise and towards the end of puberty or in early adult life, its rate of growth begins to decrease. The bone stops growing altogether when there is sufficient calcification and when the epiphyseal plates (Item 1) "fuse" or harden, thus creating physical barriers to further growth at the ends of the bone.
If during the teenage years there is a lack of testosterone or oestrogen, as found in Kallmann syndrome normal calcification cannot occur. Consequently, the epiphyseal plates do not appear until long after the normal age of puberty, fusing only partially (item 2) and occasionally failing to fuse at all (item 3).
The result is that the bones, especially those in the arms and legs, have continued to grow beyond their expected length. This can lead to unusual body proportions and bones that are weaker than their should which can lead to conditions known as osteopenia or osteoporosis.
Long arms and legs are relatively common characteristics of many forms of hypogonadism. When they appear together, this used to be and sometimes still is referred to rather misleadingly as eunuchoidism, though this term is not often used these days.
An eunuch is a male who has had his testes removed by castration and subsequently becomes hypogonadal, unable to maintain normal testosterone levels. A eunuchoid has physical characteristics resembling those of a eunuch, but these have become apparent not as a result of castration, but due to a hormonal deficiency such as that found in Kallmann syndrome. The term "eunuchoidism" is a little inaccurate because long arms and legs are not only observed in hypogonadal men (which the word "eunuchoid" implies) but also in hypogonadal women.
One medical definition of eunuchoidism is when a person's span (the distance from fingertip to fingertip) exceeds his or her height. Normally a person's span is approximately equal to their height (Fig 12) but in people with hypogonadism as in Kallmann syndrome the span can be four or five inches greater than the height.
Eunuchoidism is more common amongst those hypogonadal people who remain untreated beyond the normal age of puberty. Treatment would have allowed the bones to grow and strengthen almost normally.
One reason treatment, especially in young boys with Kallmann syndrome is not started too early is the risk of fusing the end plates too early and preventing any further growth upwards. A young teenager with suspected Kallmann syndrome might be keen to start treatment as early as possible to ensure puberty starts at the correct time but doctors have to take into account overall height to ensure treatment is only started when the person is the correct height for their age.
Sometimes an x-ray of the wrist is taken when Kallmann syndrome is suspected. This is used to assess the bone age, and to compare it to the actual age of the patient. If the bone age is too low treatment might have to be delayed for a while to allow for more growth.
People with Kallmann syndrome still experience a growth spurt sometime in their teenage years or early twenties. In people with normal testosterone or oestrogen levels it is an exponential growth in height before the testosterone or oestrogen takes full effect and stops further growth. In people with Kallmann syndrome the growth spurt is more gradual and linear as they lack the hormones to stop the growth when required.