Attending European Society of Paediatric Endocrinologists (ESPE) meeting 2024.






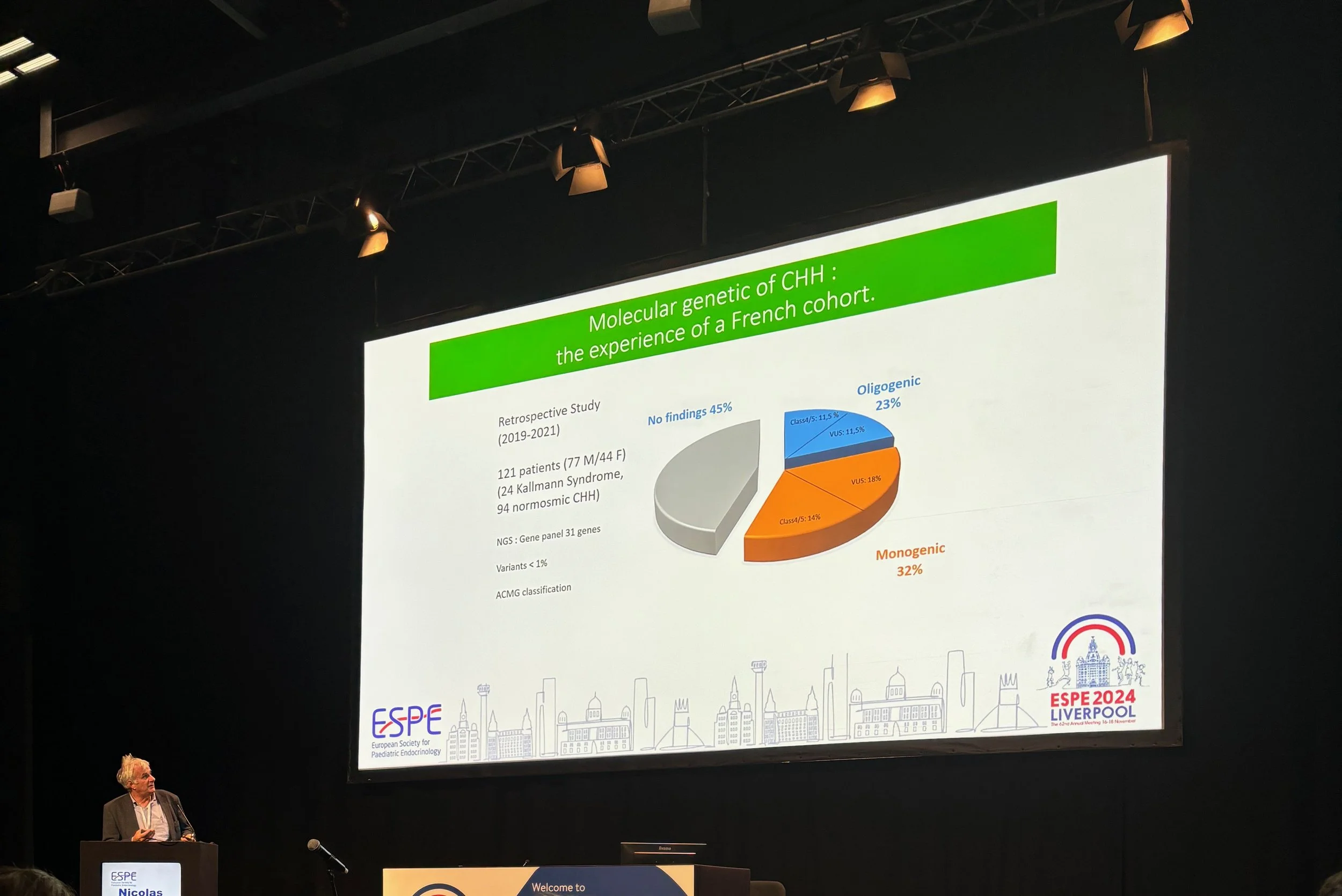















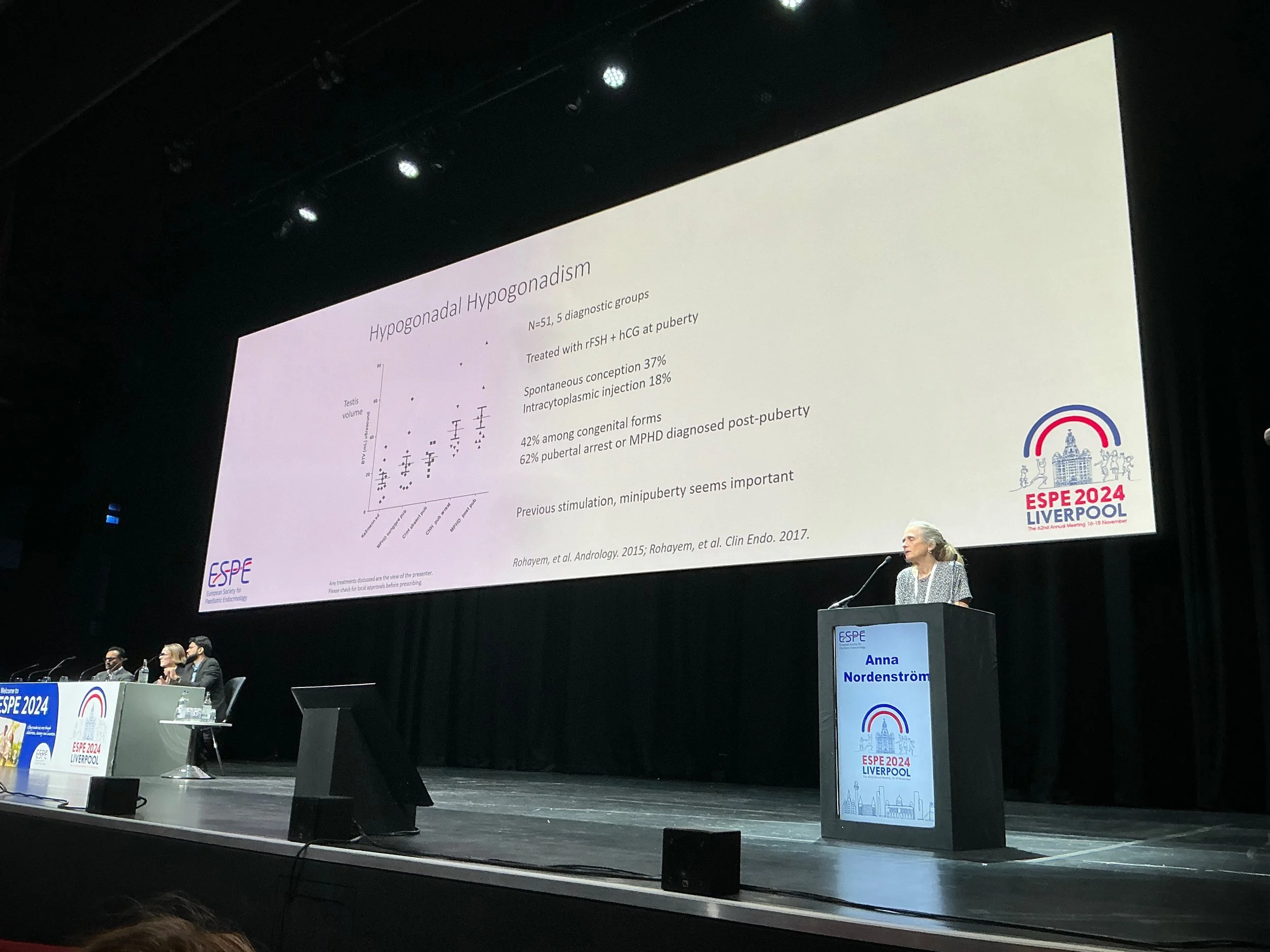


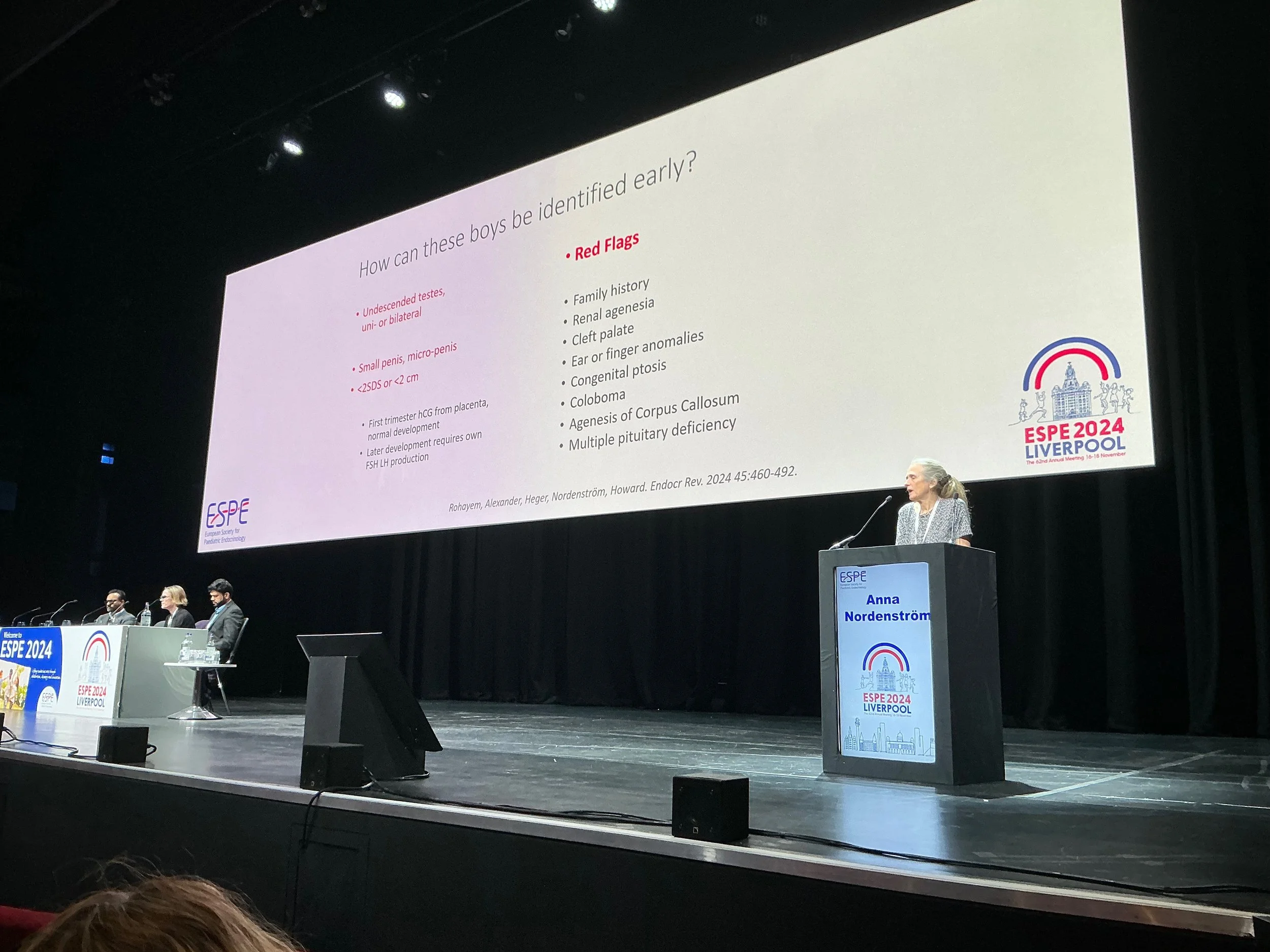









I recently attended a meeting of ESPE - European Society of Paediatric Endocrinologists in Liverpool, UK. I attended presenations relevant to Kallmann syndrome / hypogonadotropic hypogonadism.
The three presentations were on genetic testing for HH patients, mini puberty and treatment of adult HH patients.
Points of interest:
A couple of Danish studies that link low testosterone levels in mini puberty to language and social skills later in life.
The lack of hormones in mini puberty is more apparent in males than females, but can be detected in both.
The presentation on adult KS / CHH mentioned vasomotor effects as a symptom - hot flushes and sweating.
Mini puberty is important for testicular descent, penile growth and fertility chances in males.
Mini puberty is important for breast and uterine development in females, but fertility chances should not be affected.
Endocrinology Conference - Boston. #ENDO2024
In June I will be attending the Endocrine Society conference in Boston. ENDO2024.
I will be presenting a poster on my patient journey with Kallmann syndrome from late diagnosis to patient advocacy.

Hormone therapy in Kallmann syndrome / CHH neonates and young adults.
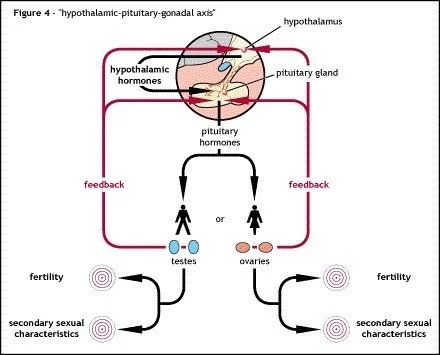
Mini puberty is the post natal surge of reproductive hormones (LH, FSH, testosterone or oestrogen) that normally occurs in the first 6 months of life.
This surge is missing in Kallmann syndrome / CHH patients.
Testing children of Kallmann syndrome / CHH parents can help in the early diagnosis of the condition if no surge is detected.
Hormone treatment before 6 months of age, in males, to replace this missing mini puberty can help in future physical development, as with penile and scrotum development. It is also thought it could help with future fertility treatments but this has left to be proved by follow up studies on patients given early treatment.
Gonadotropin can be used instead of testosterone therapy in teenage male patients. It will allow for testicular growth and potentially fertility. There may be a body image advantage in having a more natural looking puberty at this age.
It is a more intensive therapy than testosterone replacement, with more injections and can be more expensive that testosterone therapy.
The use of FSH alone first before the use of hCG in fertility treatments can mimic the missing mini-puberty. This approach is becoming standard within KS specialist centres, especially in severe cases where the initial testicular volume is low. However more research may be required and it could be many years before this approach is known and accepted by endocrinologists who do not treat Kallmann syndrome / CHH patients often.
University College Cork. School of Applied Psychology. Research Seminar. The psychological and lived experience of Kallmann syndrome.
In March 2023 I took part in a talk given at the University College Cork Applied Psychology Department.
Dr Samantha Dockray is running a research project looking at the psychological and social aspects of living with Kallmann syndrome / CHH. The first part of the project involved interviews with 14 patients (7 male and 7 female).
This video is a presentation given by a patient (me) and then Dr Dockray presents some preliminary findings of the review of the patient interviews so far.
It is hoped this will lead to future projects to help in the understanding of the psychological issues patients with Kallmann syndrome / CHH face living with their condition.
Presentation on delayed puberty v Kallmann syndrome - hypogonadotropic hypogonadism
Scientific Seminars International.
Delayed puberty: Update on Causes of delayed puberty, treatment, issues on pubertal induction protocols
Presentation posted on 3rd May 2023 given by Dr Richard Quinton of Royal Victoria Infirmary, Newcastle upon Tyne, UK.
Although primarily aimed at health care professionals, mainly paediatricians this presentation can give useful information to patients with Kallmann syndrome / hypogonadotropic hypogonadism.
It highlights the protocols used to distinguish Kallmann syndrome / HH from self correcting delayed puberty and outlines the different treatment options available.
Identifying Kallmann syndrome / HH early from self correcting delayed puberty can help in the prompt diagnosis and treatment of patients, instead of them being told to “wait and see” or being incorrectly labelled as “late bloomers”.
Patient made presentation on Kallmann syndrome.
For me the psychological issues associated with Kallmann syndrome / CHH should have more recognition.
Hormone replacement therapy can help with most (but not all) of the physical symptoms and specialised gonadtropin therapy can help some patients achieve fertility.
However the fact patients miss out on both puberty and adolescence can leave patients with symptoms that last well into adulthood. The psychsocial impact of not developing correctly can leave some patients with poor body image and social confidence problems
Since Kallmann syndrome / CHH comes with a range of symptoms and severities it can affect individual patients differently. Interacting with patient groups to communicate with fellow patients can help patients learn more about their condition and hopefully form a positive outlook.